There are several clinical situations that can cause cerebral vasospasm, but the primary reason is subarachnoid hemorrhage (SAH) due to aneurysms, arteriovenous malformation (AVM), traumatic head injury. Other conditions that may lead to vasospasm are eclampsia, postpartum encephalopathy, pituitary surgery/stroke, migraine, and drugs such as cocaine and bromocriptine.
 Figure 1: BA vasospasm
Figure 1: BA vasospasm 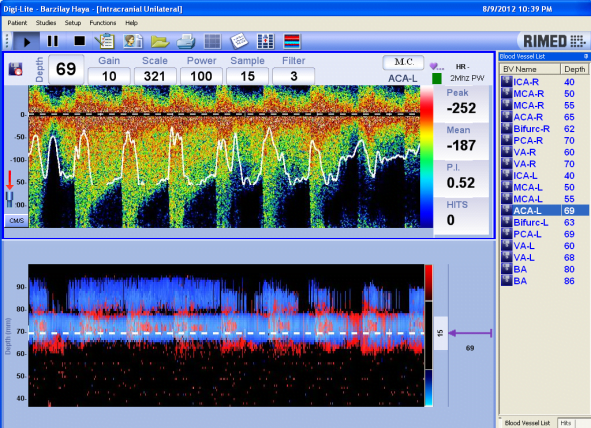 Figure 2: Left ACA vasospasm
Figure 2: Left ACA vasospasm  Figure 3: Left MCA vasospasm
Figure 3: Left MCA vasospasm Transcranial Doppler (TCD) is widely used for diagnosis and follow-up of vasospasm in neurosurgery departments and neuro-intensive care units. TCD examinations of patients with SAH are clinically relevant if performed daily (sometimes twice a day or once in two days during the critical period for the development of vasospasm, 3-15 days post-SAH).
TCD is used for cerebral vasospasm diagnosis and follow-up, according to the following criteria:
- Flow velocities:
Intracranial ICA, MCA, ACA ≥130 cm/sec
VA ≥80 cm/sec
BA ≥ 90 cm/sec
PCA ≥110 cm/sec - MFV MCA/MFV extracranial ICA >3 (Lindegaard ratio)
- MFV BA/MFV extracranial VA >2
- Changes in the Doppler waveform: decrease of pulsatility index (PI), signs of turbulence, fluttered envelope
- Rapid early rise in flow velocities (more than 25% per day)
- In severe vasospasm: decrease of flow velocities with progressive weakening of the signal
The advantages of using TCD for cerebral vasospasm diagnosis are:
- Noninvasive
- Comfortable, bedside examination
- Easily repeatable examination (can be performed daily)
- Enables easy follow-up for vasospasm
- Cost-effective
- High sensitivity and specificity
- Enables early detection
TCD is the only noninvasive technique with high sensitivity and specificity. It is an uncomplicated, easy-to-use tool for cerebral vasospasm diagnosis and follow-up.